Review the 2024 TCCC Guidelines.
Look for TCCC Courses at www.911tacmed.com
#tccc
Look for TCCC Courses at www.911tacmed.com
#tccc
|
Review the 2024 TCCC Guidelines. Look for TCCC Courses at www.911tacmed.com #tccc
0 Comments
National Component Requirements Expiration dates through Sept. 30, 2025: Download the 2016 NCCP Model (PDF) Expiration dates on or after March 31, 2026: Download the 2025 NCCP Model (PDF) This is for everyone who is an EMR, EMT, A-EMT, and NRP to see where your hours count and the minimum required hours to recertify. For Scheduled Training please to go www.911tacmed.com and scroll down to mid page. Also, you can find level-specific information on the recertification pages for: EMR: https://nremt.org/EMR/Recertification EMT: https://nremt.org/EMT/Recertification AEMT: https://nremt.org/AEMT/Recertification Paramedic: https://nremt.org/Paramedic/Recertification Global Pandemics: Gain-of-Function Research of Concern by the Congressional Research Service (CRS).24/11/2022 Tactical Combat Casuatly Care (TCCC) 2 Day Course with Ballistic Wound Packing Lab, Lung & Airway Labs Sat, Feb 26 - Sun, Feb 27, 2022 8:00am-5:00pm 11641 I-35W N, Grandview, TX 76050-3522, United States Tactical Combat Casualty Care BRING YOUR TACTICAL KIT & (Weapon not required / optional) AND BE READY TO LEARN AND GET DIRTY! If you have NVGs bring them for optional night training. We have Plate Carriers and Armor if you do not have your own. TCCC with ballistic wound packing lab, lung and airway lab The Tactical Combat Casualty Care (TCCC) course introduces evidence-based, life-saving techniques and strategies for providing the best trauma care on the battlefield. NAEMT conducts TCCC courses under the auspices of its PHTLS program, the recognized world leader in prehospital trauma education. NAEMT’s TCCC courses use the PHTLS Military textbook and are fully compliant with the Department of Defense’s Committee on Tactical Combat Casualty Care (CoTCCC) guidelines. It is the only TCCC course endorsed by the American College of Surgeons. The TCCC-MP (TCCC for Medical Personnel) course is designed for combat EMS/military personnel, including medics, corpsmen, and pararescue personnel deploying in support of combat operations. NAEMT’s TCCC course is accredited by the Continuing Education Coordinating Board for Emergency Medical Services (CECBEMS) and recognized by the National Registry of EMTs (NREMT). Almost 90% of American service men and women who die from combat wounds do so before they arrive at a medical treatment facility. This figure highlights the importance of the trauma care provided on the battlefield by combat medics, corpsmen, PJs, and even the casualties themselves and their fellow combatants. With respect to the actual care provided by combat medics on the battlefield, however, J. S Maughon noted in his paper in Military Medicine in 1970 that little had changed in the preceding 100 years. In the interval between the publication of Maughon's paper and the United States’ invasion of Afghanistan in 2001, there was also little progress made. The war years, though, have seen many lifesaving advances in battlefield trauma care pioneered by the Joint Trauma System and the Committee on Tactical Combat Casualty Care. These advances have dramatically increased casualty survival. This is especially true when all members of combat units – not just medics - are trained in Tactical Combat Casualty Care (TCCC.) Cost: $400 You must notify us to pay and reserve a training seat. Call if you have anyquestions or to submit payment: 270-871-2953 Where: 11641 I-35W N, Grandview, TX 76050-3522, United States Credit: 16 hours TCOLE Credit 16 hours Medical CEUs • Host Hotel: Comfort Suites Hotel (817) 293-7900 400 Village Park Dr., Alvarado, TX 76009 Rate Code: RANGE 35 Rate: $59.00 King - $69.00 double queen Course info can be found on the www.911tacmed.com homepage #tccc #deplymentmedicine #911tacmed #combatmedic #68W #pj #corpsman #military #ems #leo #fire #police 26 FEB IBSC TACTICAL PARAMEDIC (TP-C) & TACTICAL RESPONDER (TR-C) REFRESHER COUSRSE Sat, Feb 26 - Sat, Mar 5, 2022 11641 S. Interstate 35W, Grandview, TX 76050 TP-C & TR-C Refresher Course 26 FEB Tactical Combat Casuatly Care (TCCC) 2 Day Course with Ballistic Wound Packing Lab, Lung & Airway Labs Sat, Feb 26 - Sun, Feb 27, 2022 8:00am-5:00pm 11641 I-35W N, Grandview, TX 76050-3522, United States Tactical Combat Casualty Care 26 FEB TEMS / Basic SWAT Tactical Medic Course Sat, Feb 26 - Fri, Mar 4, 2022 8:00am-5:00pm 11641 S. Interstate 35W, Grandview, TX 76050 Basic SWAT Medic Course 28 FEB Basic SWAT Course by Special Operations Systems Mon, Feb 28 - Fri, Mar 4, 2022 10:00am-10:00am 11641 I-35W Frontage Rd, Grandview, TX 76050 [email protected] 7 MAY TEMS Advanced SWAT Medic (MUST HAVE COMPLETED BASIC TEMS OR EQUIV) Sat, May 7 - Wed, May 11, 2022 All day 11641 S. Interstate 35W, Grandview, TX 76050 Advaned SWAT Medic for the Tactical Operators If you Agency or Department needs any K-9, Medical or Tactical Training for TCOLE, Medical CEs, or Proficiency Training do not hesitate to contact us at [email protected] , [email protected] or call 270-871-2953. Find more training on the homepage of www.911tacmed.com #training #Medical #tactical #SWATMedic #Tactical Paramedic #TCCC #TCOLE #911tacmed CategoriesFREE TCCC Card DD-1380 $0.00Get your free download for TCCC Cards / DD-1380. This stuff is free so please take it and download it here, print it off and laminate of if you need to, punch a hole in it and put a rubber band on it. After words put that sucker in your IFAK and your teams IFAKs. Then go get a sharpie (small one) and you are set. he DD Form 1380, TCCC Card is the standardized method for documentation of casualty care in the prehospital environment for battle and non-battle injuries. The DD Form 1380 promotes Department of Defense goals of capturing documentation of pre-hospital medical interventions at the point-of-injury. First responders, to include clinical providers, will document treatment using the current TCCC guidelines. ADDITIONAL INFORMATION This content was designed for use in the Tactical Combat Casualty Care for All Service Members Course (TCCC ASM), and is intended for nonmedical personnel. The Joint Trauma System (JTS) establishes the standard of care for prehospital battlefield medicine for the Department of Defense. The JTS is part of the Defense Health Agency providing clinical practice guidelines and performance improvement for all levels of military trauma care. The JTS is supported by the Committee on Tactical Combat Casualty Care (CoTCCC) which is composed of representatives from across the Army, Navy, Air Force and Marines develops clinical practice guidelines for the delivery of Tactical Combat Casualty Care (TCCC) on the battlefield. For all your medical training needs and real-world mission needs feel free to reach out to us at www.911tacmed.com #TCCC #Documentation #CoTCCC #TacticalMedicine #Emergency #tacticalParamedic, #DD1380 #TECC #Tacmed #Fire #EMS #EMT #911tacticalmedicine #documentation FREE TCCC Card DD-1380
$0.00
Get your free download for TCCC Cards / DD-1380. This stuff is free so please take it and download it here, print it off and laminate of if you need to, punch a hole in it and put a rubber band on it. After words put that sucker in your IFAK and your teams IFAKs. Then go get a sharpie (small one) and you are set. #TCCC #Documentation #CoTCCC #TacticalMedicine #Emergency #tacticalParamedic, #DD1380 #TECC #Tacmed #Fire #EMS #EMT Here at 911 Tactical Medicine, we do a lot of training and teaching others about some serious real-world situations. A lot of the time some of the minor things get over looked, even though they are just as important. We want to start publishing articles on some of the more common things around us. Anything from allergies to a sprained ankle, we want to cover all areas of education to help you.
Injuries and Back Pain Injuries can cause back torment, including injuries to the upper appendages, shoulders, neck, spine, and so forth Injuries can happen likewise cause back torment if the rotator sleeves are upset. The rotator sleeves contain acromion, ligaments, for example, the rotator sleeves, which rest at the upper bones at the arm, and associate with rotator sleeve muscles. The muscles are at the highest point of the upper arm bones, and beneath the shoulder joints. Rotator sleeves are bunches of more modest muscles, ligaments, and so on, and join to different pieces of the body. On the off chance that the ligaments are torn or potentially burst it can cause back torment. The injuries as a rule happen when unexpected effects or powers focus on the district. Applying the muscles can likewise cause injury. On the off chance that the ligaments are harmed, it causes aggravation and expansion, which makes a large amount of pain. Such issues are treated with rest, ice packs, pressure, and elevation. Shoulder injuries are seen when the arm is tossed out of attachment. The injuries happen from falls, overexerting muscles, and so forth. The specialist considers such injuries carefully since breaks might emerge, which begin inside the humerus. In certain occurrences, medical procedure is mandatory to address the issue. Additional injuries incorporate circular segment pain, shoulder freeze, tendonitis, subacromial bursa, acromio-clavicular, etc. The Bursa is a sac loaded up with liquids that fill in as cushioning to diminish friction. The reason for the bursa is to make development simple and to deflect scouring of the joints. The bursa can cause issues when the shoulders are out of nowhere thrown over the head. Treatment for subacromial bursa conditions, incorporate steroid regimens, exercise-based recuperation, prescriptions, and so forth, particularly when aggravations set in. The condition can cause back pain since the bursa is an aide to the joints, ligaments, bones, and synovium. Bursa works by making light of the dangers of joint harm. On the off chance that bursa kindles it packs the nerves or ligaments. What occurs after is a disappointment, particularly once the joints rub. The delicate pockets amid the bones that cover and ensure different bones can cause genuine back torment since aggravation has set in from bursa problems. The strain caused by aggravation hits the muscles, overexerting these muscles, which the tangible nerves are dialed back and development is restricted. Stance is the posture we get from bearing muscles and joints. If an individual slouches, regularly it can cause back pain, since the muscles and joints are not moving, as they ought to. Active recuperation and medications are frequently utilized to address the issue. Sitting at long spans can likewise cause back issues, particularly if the lower back isn't upheld. Indeed, sitting erroneously can twist the spine at the lower back and cause genuine agony. Back torment in this nature might show up from sport exercises also, for example, truly difficult work, continued curving, etc. Slouches can address back issues by figuring out how to sit and remain in legitimate positions. The back when harmed from slumping influences the lumbar. Furthermore, the slouchier should learn the right methods of lifting. Back pain can show up from the slipped circle, sciatica, Sacro-iliac, and so forth Slip circles are a Herniated core pulposa (HNP) jumble. Slip circles are bursting of the "intervertebral plate." The intervertebral circle sits amid the Spinal Columns and is close to the spine. Profoundly, lastly at the disk. At the point when the nerve roots are compelled, the disk can slip, causing herniated core pulposa. Sciatica is a kind of slipped disk, since the aggravation sends sharp, electrical shock-like agony down the waterway of the spine, sending an upsetting hurt that begins in the back. The aggravation conveys onto the legs. The aggravation is now and again discontinuous, yet on different occasions, it can prompt ongoing torment condition. Surgeries are frequently needed to address the issue. Published by, Michael Taylor Head of 911TacMed - Networking - Marketing - Social Media - Web Managemen US Army Ret. CEO TaylorLyfe Digital Marketing 911 TacMed Website: www.911tacmed.com Facebook: https://www.facebook.com/911TACMED LinkedIn: https://www.linkedin.com/company/911-tactical-medicine YouTube: https://www.youtube.com/channel/UCHM_WFJAeVy2t40CsT11Pqw/featured Get your free download for TCCC Cards / DD-1380. This stuff is free so please take it and download it here, print it off and laminate of if you need to, punch a hole in it and put a rubber band on it. After words put that sucker in your IFAK and your teams IFAKs. Then go get a sharpie (small one) and you are set.    Please Share With Anyone Who May Need Them.
Every time you buy 3-ply face masks with Mask Challenge USA, we will donate masks and Personal Protective Equipment (PPE) to our everyday heroes: frontline volunteers, medical workers, and first responders. Step 1. You buy a 20 or 50 pack of 3-ply, non-medical masks through Mask Challenge USA website for yourself and your family. Step 2. Mask Challenge USA donates Personal Protective Equipment (PPE) to support those who support our community: volunteers, medical workers, first responders. BUY Masks Buy MasksWhy buy masks online from Mask Challenge USA?
Nominate NominateNominate an Everyday Hero! Do you know of a worthy group of everyday heroes who need masks? Nominate the volunteer group or organization below for a chance to receive 500 3-ply masks from Mask Challenge USA. Please note: We're excited to donate to as many everyday heroes as possible but please know that due to the high volume of need, we are unable to accommodate all requests. Thank you so much! This is why we train and stay ready. This is the difference between 2 and 24 killed. Church shooting today near Fort Worth Tx. Bad guy in black with shotgun (red) gets killed by good guy and parishioner with LTC (green). Clearly this could have ended so much worse. That’s a solid distance to shoot a pistol under stress. Good work! Make sure you have trained staff and kits to treat people afterwards. If you need help let us know. If we cant get you what you need we will point you in the right direction or find someone else who can. Train hard because dying sucks. #thingsthatmatter #training #emt #medic #leo #police #chl #shooter #stayready #tragedy #education #medical #tactical #stopthebleed #bleedingcontrol #shootingclass #pistol #school #church #trainhardbecausedyingsucks #goodpeople #Texas  Check out the Spring 2018 Combat & Casualty Care magazine put out by Defense Media. Matthew Kinney our CEO wrote a little article that was three pages with picture. Those pictures where of him doing a Rescue Hoist mission in the Korengal Valley, Afghanistan, Training Soldiers in TCCC and PFC, and last is one of his critical care patients that had a gunshot wound to the right side of the head who was ventilated in Iraq. Take a read through the magazine and make sure to read the" "EVOLVING “GOLDEN HOUR” CARE TO MITIGATE THE TREATMENT GAP" 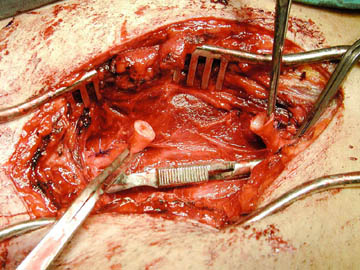 Image for reference Had a first Friday night that I thought you’d appreciate. Had a male patient that was attacked with a sword to the left shoulder/chest. It was medial enough you couldn’t get a tourniquet on it. EMS had tried to control the bleeding with direct pressure but couldn’t get it stopped. The sword had created a large defect which made it difficult to obtain source control. The surgery resident tried to pack the wound with quik clot but it became obvious he wasn’t sure how to do it as he just laid the dressing in the wound bed. So, in the trauma bay I gave him 25mg of Ketamine for a little cooperation. Then I packed the wound with the quik clot followed by two rolls of Kerlex to completely fill in the defect and get enough pressure to control the hemorrhage. It was difficult because of the sheer size of the injury, not necessarily hidden cavities. At the same time, he got a gram of TXA as we took him to the OR. In the OR it was explored and it turned out he’d severed a branch off the subclavian. Thanks for the training and experience. Brian Brian was in one of our Basic SWAT Medic Courses We love to hear feedback from our students and how the training has help them. This is just one of the many we sharing. Please watch and share the touching story of the 173rd Airborne during the Battle of Wanat. Matthew Kinney helped save the lives of these men and wants everyone to hear their story as they tell it. This film is a True Life Documentary, Narrated by the soldiers of Chosen Company 2nd Platoon 173 Airborne  Your gloves play a vital role in your patient assessment. Black gloves greatly reduce that ability to identify blood. This is especially true in low light / no light situations with or without supplemental lighting.  Come see us at #booth 421 at the #TexasStateEMSConference Nov 19-20. We will also be at the #preconference Nov 18-19 conducting our #TCCC course. Those who wish to take their Tactical Responder Exam will be eligible to after our #course for #free if you are not a paramedic. Those that are #paramedic certified will be eligible for the #TacticalParamedic Exam but we have to register and pay for their exam through the #IBSC The Great American Shoot & Donations for the Special Forces Charitable Trust (100% of all donations go back to SFCT) |
|||||||
| | |
| tccc.pdf |
| tccc_quick_reference_guide.pdf |



Blog and Articles
June 2024
February 2024
November 2022
October 2022
August 2022
May 2022
January 2022
December 2021
December 2020
May 2020
December 2019
March 2019
May 2018
November 2017
October 2017
September 2017
August 2017
July 2017
June 2017
May 2017
April 2017
March 2017
February 2017
January 2017

|

|
 RSS Feed
RSS Feed