|  |
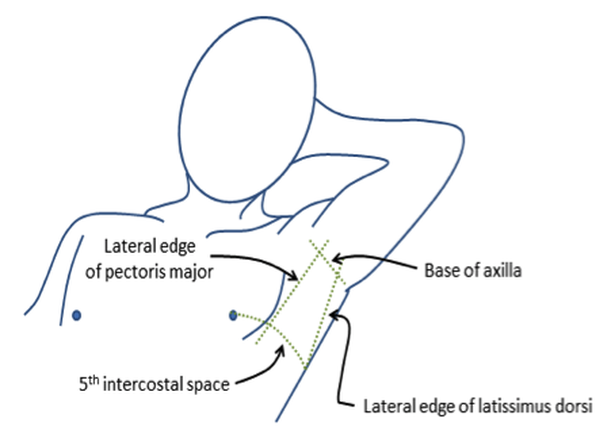
A 23 year old, 230 pound, muscular, African-American active duty (AD) Soldier in the U.S. Army sustained a high-velocity gunshot wound to his left shoulder in Paktika, Afghanistan. The projectile penetrated anteriorly, immediately inferior to the distal 1/3d of the left clavicle and exited inferior to the left scapula. He was treated by a first responder AD 68W Combat Medic with two packs of QuickClot Combat Gauze (Z-Medica, Wallingford, Connecticut, USA). The gauze was packed into the wound under direct pressure and an 18g IV was placed in his contralateral upper extremity. An infusion of 0.9% normal saline (NS) was initiated at a slow rate. He arrived at the 9 man surgical element, we bypassed EMT and just brought him straight into the OR.
After preoxygenation with 100% oxygen, a Sellick’s maneuver was applied to the patient’s cricoid cartilage and induction of general anesthesia was achieved with Etomidate (Amidate, Pfizer, Inc., New York, USA) followed immediately with succinylcholine (Anectine, Quelicin, suxamethonium, Pfizer Inc., New York, USA). Direct larnygoscopy was performed, a Grade I view was obtained, and an 8.0mm endotracheal (ET) tube was inserted between the true vocal cords to a depth of 22cm at the teeth. The ET cuff was inflated with 5mL of air and breath sounds were equal bilaterally with a positive end tidal CO2 waveform on the monitor (Propaq, ZOLL Medical, Chelmsford, Massachusetts, USA).
After verification of ET tube placement, a massive amount of blood was noted on the floor. Upon inspection, the patient had a rapid, active, arterial flow of pulsatile blood emanating from his wound. An entire roll of gauze (Kerlix, Covidien,-Medtronic, Minnesota, USA) was placed into the wound and direct pressure was applied. The patient was placed on the ventilator.
The patient was found to have a partially severed left subclavian artery.
Succinylcholine is a widely used medication as part of the RSI technique in combat casualties. Application of Combat Gauze to penetrating injuries has become routine for U.S. military forces. The fasciculations caused by succinylcholine can be of sufficient intensity to dislodge the Combat Gauze and result in a rapid loss of hemostasis. Alternatively, an actively moving patient can dislodge the clot formed by combat gauze.
I recommend a reinforcing combat gauze prior to patient movement, using a defasciculating dose of paralytic prior to using succinylcholine, or avoiding succinylcholine altogether if the patient has had a hemostatic dressing applied. The patient also received 4u PRBCs and 4 FFP, we didn't have TXA during surgery.
-George Johnson
CRNA
After preoxygenation with 100% oxygen, a Sellick’s maneuver was applied to the patient’s cricoid cartilage and induction of general anesthesia was achieved with Etomidate (Amidate, Pfizer, Inc., New York, USA) followed immediately with succinylcholine (Anectine, Quelicin, suxamethonium, Pfizer Inc., New York, USA). Direct larnygoscopy was performed, a Grade I view was obtained, and an 8.0mm endotracheal (ET) tube was inserted between the true vocal cords to a depth of 22cm at the teeth. The ET cuff was inflated with 5mL of air and breath sounds were equal bilaterally with a positive end tidal CO2 waveform on the monitor (Propaq, ZOLL Medical, Chelmsford, Massachusetts, USA).
After verification of ET tube placement, a massive amount of blood was noted on the floor. Upon inspection, the patient had a rapid, active, arterial flow of pulsatile blood emanating from his wound. An entire roll of gauze (Kerlix, Covidien,-Medtronic, Minnesota, USA) was placed into the wound and direct pressure was applied. The patient was placed on the ventilator.
The patient was found to have a partially severed left subclavian artery.
Succinylcholine is a widely used medication as part of the RSI technique in combat casualties. Application of Combat Gauze to penetrating injuries has become routine for U.S. military forces. The fasciculations caused by succinylcholine can be of sufficient intensity to dislodge the Combat Gauze and result in a rapid loss of hemostasis. Alternatively, an actively moving patient can dislodge the clot formed by combat gauze.
I recommend a reinforcing combat gauze prior to patient movement, using a defasciculating dose of paralytic prior to using succinylcholine, or avoiding succinylcholine altogether if the patient has had a hemostatic dressing applied. The patient also received 4u PRBCs and 4 FFP, we didn't have TXA during surgery.
-George Johnson
CRNA

 RSS Feed
RSS Feed